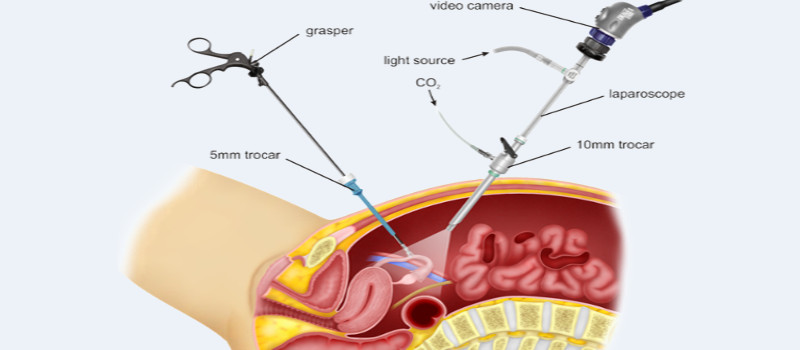
Specialised instruments that can be passed through tiny cuts made in the abdominal wall and the use of magnification using optics and camera, creation of pneumo peritoneum to distend the abdomen have made key hole surgery possible.
It gives access to deeper organs inside the belly.
Kidneys which are totally damaged by longstanding blockage, stone can be removed by this method. The destroyed kidney is separated from its vascular and tissue attachment and is then removed.

Kidney tumour starts as a small swelling and increases in size gradually. There may not be any symptoms initially but symptoms of passing blood in the urine, pain in the lateral side of abdomen will gradually appear. Tumour is best diagnosed with CT scan with contrast injection.
If the tumour is more than 4 cm, the entire kidney along with the surrounding fat is removed to give a good cancer cure. This is called Radical nephrectomy.
If the tumour is small 2 cm or slightly more and multiple, the tumour along with surrounding segment of normal tissue can be removed to provide cure. The remaining normal kidney tissue is preserved. This is called partial nephrectomy.
The blockage site pelviureteric junction (Junction of outlet of kidney and ureter) can lead to poor urine drainage from the kidney and the urinary system swells up leading to reduced kidney function. By removing the narrow segment and restoring continuity kidney function can be restored.
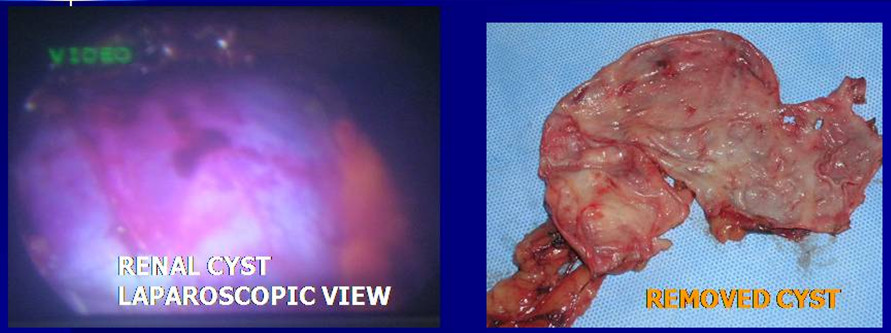
Small renal cysts are commonly seen on routine scan. They are harmless and only follow up is require annual follow up scan Larger cysts over 6 cm are prone to stone formation, cancer developing within it and may rupture causing acute pain. They are best removed laparoscopy. The cyst wall is removed completely and kidney is safeguarded.
Adrenals are deeply placed just above the kidney like a cap. Laparoscopy is best suited to manage swelling or tumour arising from adrenals.

Normally both testis should be present in the scrotum. When the testis fail to descend to its normal location they can remain within the abdominal cavity or in the groin. These undescended testes carry risk of rotation, pain (Torsion) and may develop cancer within the testis. Laparoscopy can easily identify the location aed in the scrotal area (Orchidopexy) if the testis is present but riny, they can be removed laparoscopically.
Large renal cysts can cause pain, bleeding and rarely can harbour cancer within the cyst. They are also prone to rupture causing sudden severe abdominal pain.
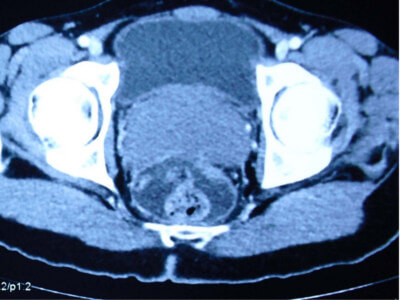
The mullerian duct cyst is a congenital condition represents remnant of the caudal ends of the fused müllerian duct, a structure that typically regresses in time. These cysts are typically located in the midline, behind the bladder, originating in the region urinary passage just below the level of prostate connected by a thin stalk. It is not associated with other congenital abnormalities of the urinary tract. The cystic fluid is devoid of sperms, and may be thick tenacious or sometimes blood stained. Rarely stones may occur within these cysts. It is common between 20 to 40 years.
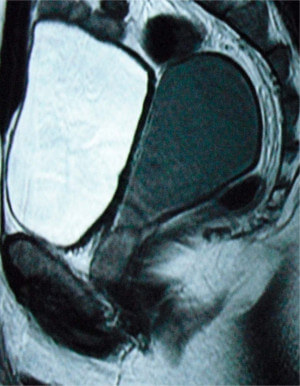
The clinical presentation is varied, including urinary frequency, urgency, dysuria, urinary obstruction, hematuria, and pelvic pain. Digital rectal examination may reveal a midline mass superior to the prostate gland. Transrectal ultrasound and MRI will confirm the diagnosis.
These large cysts can be removed by laparoscopic surgery.
© Copyright 2024 | Powered By Tech Thulasii



